
IE

By Declan Kelly, Founder & CEO, Eolas Medical Reading time: ~10 minutes
Stand next to a clinician at any clinical encounter and watch what happens in the thirty seconds before a decision.
They are listening to the patient. They are scanning the chart for what's already known i.e. comorbidities, medications, recent results, the last note etc. They are running an internal mental search across everything they remember about evidence, guidelines, the local pathway, and even what their colleagues would do. And then, in that compressed moment, they decide on a path forward that informs this patient’s clinical journey.
Three streams of information. One moment. One starting point for the trajectory of their decision making processes moving forward..
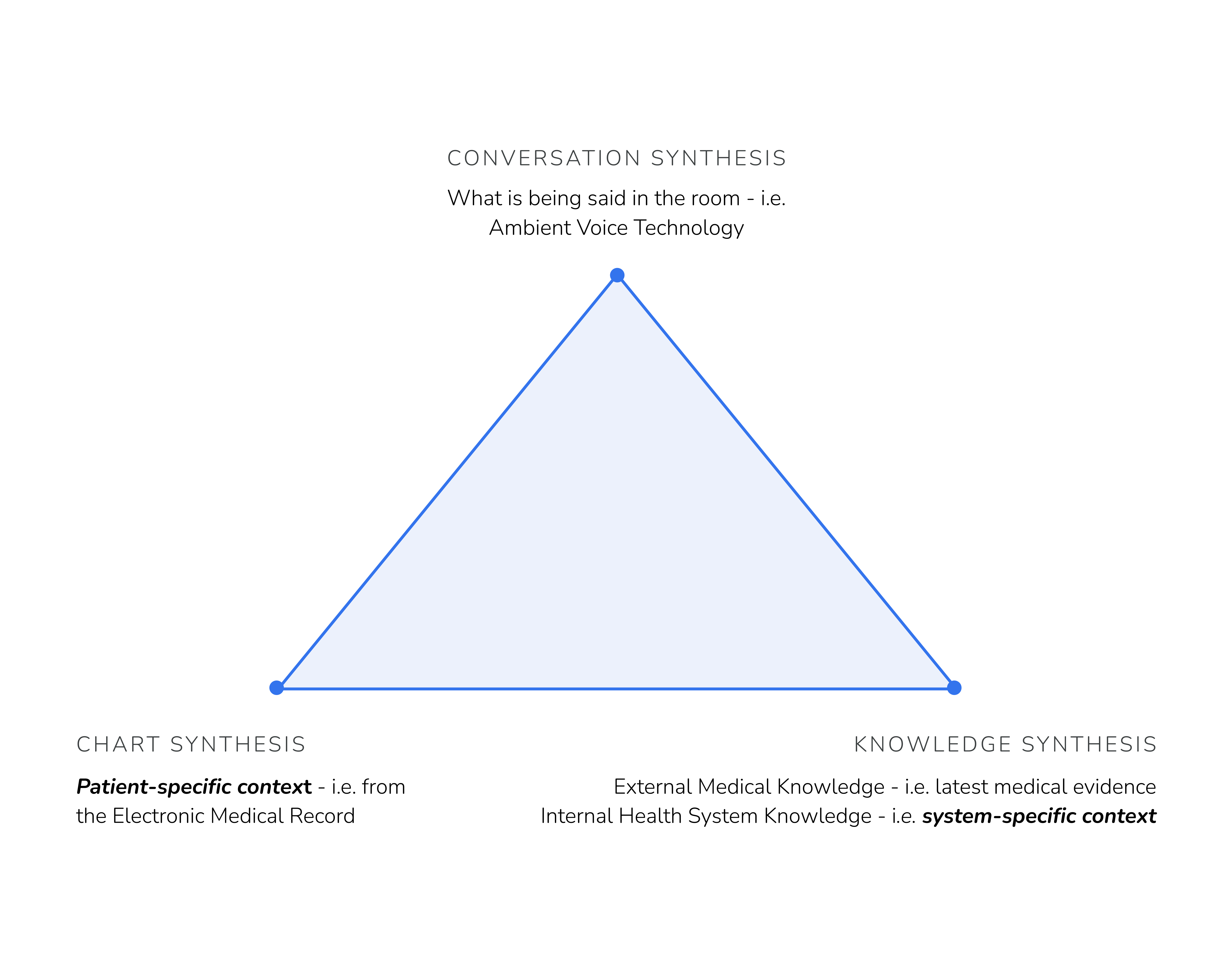
This is what clinical AI is also evolving towards. Not in isolation, better dictation, better search, better charting, the destination is the integration of these three streams, synthesised in real time, into a trusted clinical path forward, for that patient, in that health system.
These three elements, i.e. conversation synthesis, chart synthesis and knowledge synthesis form three points of a “Golden Triangle” of clinical AI.
Each corner is a distinct technical, commercial and clinical problem. Each has its own emerging category leaders. Each is at a different stage of maturity. And each has limiting factors that are holding the whole triangle back from being realised.
This piece takes a journey, walking to each corner: what it is, where it stands today, what's stopping it, and what has to change for the integrated future to arrive.
What is being said in the room.
Conversation synthesis is the act of listening to a clinical encounter, transcribing it, and turning the transcript into a structured clinical note. Ambient AI scribes are the wedge product. A microphone in the consultation room captures the doctor–patient conversation. A (usually fine-tuned) large language model takes the raw transcript and writes a clinical-grade note in the right format, with the right structure, in under a minute.
The most mature corner of the triangle. Microsoft's DAX Copilot is deployed in 600+ healthcare organisations. Abridge has signed 200+ US health systems including Mayo, Duke, Johns Hopkins, UPMC and Kaiser. Suki, Ambience, Heidi, Nabla, Freed and a long tail of others are competing hard in the same space. When a health system offers ambient AI widely, 20–50% of offered clinicians adopt it, with best-in-class deployments hitting 75–80%. After-hours documentation time is measurably shorter. Burnout has dropped from 51.9% to 38.8% in published trials.
In adoption terms, this is the early majority and consolidation is starting to happen. Most forward looking players in the space are journeying to the other corners of the triangle at this point.
The technology is impressive, evolving fast but extremely immature in how it is implemented across and within systems. It’s quoted that modern LLM-based scribes report overall “error rates” of 1–3%, in my opinion this is not extremely relevant or the limiting factor at all, take for example a high sensitivity troponin taken at ~3hrs post chest pain, this will be ~98% sensitive for detecting myocardial damage in the case of a NSTEMI (heart attack), this isn’t perceived as having a “2% error rate” because the technology i.e. the test itself is not used in isolation, it is combined with either clinical scoring systems, internal protocols for cuts offs and serial troponin testing over time. The point here is that the intervention i.e. is only as safe and efficacious as the system it is used within. Ambients have opened up a whole new world of distinct failure modes that didn't exist before and we’re only beginning to understand these.
The position on regulation is also evolving but somewhat grey in many geographies, other geographies have clear and a firm stance on the status of these as medical devices, further helping to consolidate those markets to a few dominant players.
There are also further workflow limitations. Ambient AI works extraordinarily well in long-form consultations and outpatient settings. It struggles with multi-speaker ward rounds, theatre lists, emergency department triage, and any environment where the "conversation" is fragmented across multiple short interactions with different people. Most published outcome data is from outpatient primary care and specialty clinics, generalising to acute care is still an open question.
Lastly, how to buy it? Every geography is different with wide ranging reimbursement mechanisms, everything from clinician-led “product-led-growth” adoption with platforms like Heidi where individual clinics are paying for this out of pocket, to hundreds of millions of pounds procurement frameworks being established in the UK to help streamline health systems in their procuring of this software, but again the “how to buy it” bit is also still quite immature.
Conversation synthesis is the essential wedge to enable all other corners of the triangle to occur almost automatically if implemented correctly. The failure modes are starting to shrink to a level health systems can defend medico-legally as currently no vendor accepts clinical liability for note content. Second, the output stops being just a clinical note and becomes a structured input that the rest of the triangle can use, capturing not just words but symptoms, intent, and the clinical question the clinician is implicitly asking. Third, the corner integrates with the chart and knowledge corners so the conversation can be enriched by what the system already knows about the patient and what the system can answer in real time.
The leading vendors are all building toward this. The conversation corner is no longer the destination; it is the starting point.
What is known about this patient.
Chart synthesis is the act of taking a patient's record and turning it into something a human can absorb in seconds. Comorbidities, recent results, current medications, recent admissions, free-text notes from other clinicians, social history, allergies, pulled from across the EHR, structured, summarised, surfaced.
The corner with the most aggressive new investment in 2026. The EHRs themselves are now building chart copilots (Epic, Oracle Cerner). The ambient vendors are extending sideways from the conversation corner, Abridge, DAX and others are integrating chart context into their note workflows. The external knowledge engines are extending in from the other side, OpenEvidence's enterprise Epic deployments at Sutter Health, Mount Sinai (across seven hospitals) and Cedars-Sinai now bring patient context into the answer engine as well as their “Visits” ambient listening feature for recording the consultation.
This corner is partially built. The picture is incomplete, but working versions are starting to appear at leading academic medical centres.
Chart synthesis runs into harder problems than conversation synthesis because the underlying data is messier. Health system EHRs were not built to be summarised. They were built to be billable, auditable, and legally defensible. Procedure codes are not exhaustive, they only capture billable elements. Important clinical information lives in free-text notes that are inconsistent in length, structure, and quality. Data quality varies enormously across departments and across institutions. Interoperability across EHRs is improving with FHIR but is far from solved.
The published evaluation evidence reflects this. In one 2026 npj Health Systems study of EHR-integrated AI chart review, physicians reported positive overall impressions but flagged omissions as the most common concern, alongside token-window limitations, confusing content, and occasional hallucinations. The summaries were "acceptable for use in clinical workflows" but not yet trusted enough to act on without review.
There is a deeper limit too. A chart summary is only as good as what's actually in the chart. When a patient has been seen across multiple institutions, when imaging was performed off-site, when the consultant's verbal handover never made it into a written note, the chart is incomplete. Chart synthesis can summarise what's there. It cannot summarise what isn't.
Chart synthesis becomes part of the triangle when the corner moves from summarising the chart to understanding the patient. That requires (a) cross-institutional data sharing genuinely working, not just being technically possible; (b) AI that knows what it doesn't know and flagging gaps in the record rather than confidently summarising around them; (c) tight integration with the conversation corner, so what the patient says in the room can be reconciled with what the chart says about them; and (d) integration with the knowledge corner, so the patient's history can be queried against both the world's evidence and the health system's own protocols.
Of the three architectural approaches racing into chart synthesis, the one that wins will probably be the one that expands outward to the other corners best not the one that builds the deepest single-vendor stack, i.e. this is left up to EPIC, Cerner and the other leading EHRs to commit to building (or partnering) with actually decent Ambient Voice Technology and decent evidence/knowledge integration, so far there has been enough “sprinkling of AI” throughout the EHR to keep CMIOs happy i.e. stopping the Ambient Voice Technology players having any look in as a meaningful contender of up-ending the market. I expect this trend will continue, after all since the inception of EPIC it has seen essentially zero health systems churn from using it.
What medicine knows.
External knowledge synthesis is the AI answer engine for the world's published medical literature: peer-reviewed papers, clinical guidelines, drug references, and the formal evidence base every clinician was taught to practise from. Take a natural-language clinical question, retrieve from the global corpus, synthesise a cited answer in seconds.
The category that has scaled fastest. OpenEvidence reaches more than 50% of US physicians and went enterprise-wide inside Epic at Sutter, Mount Sinai and Cedars-Sinai through the spring of 2026. UpToDate (Wolters Kluwer), Doximity and a long tail of geography-specific competitors are racing into the same category from different starting points. OpenAI, Anthropic and Elsevier are all building adjacent products on the same external corpus.
This corner is in the early-to-late majority of adoption as a stand-alone technology. The technical problem is largely solved. The competitive dynamics are now about distribution, EHR integration, and which vendor earns the right to be the default answer engine inside each enterprise.
External knowledge engines are extraordinary at a specific kind of question and weaker at others. They excel when the clinical question maps cleanly to the published evidence i.e. diagnostic criteria, drug indications, well-studied conditions, recent randomised trials. They are weaker when the question requires synthesis across overlapping guidelines, when guidelines themselves disagree, or when the evidence base is heterogeneous, contested, or absent. Fundamentally it completely falls apart when trying to contextualise an answer specifically for that health system as process, protocols, available diagnostics and formularies all vary across different systems.
Three structural limits are worth naming.
First, geography. The global corpus of medical evidence is dominated by US- and English-language sources. A UK clinician asking about hypertension management may receive an answer grounded in the JNC guidelines rather than NICE. An Irish prescriber may get FDA dosing rather than HSE formulary guidance. The engine cannot know which geography the clinician is practising in unless it is told and even when it is told, the underlying retrieval bias remains.
Most importantly however as mentioned, external knowledge engines will give the same answer in every hospital in the world. By definition. It is what medicine knows. It is not what this health system practises.
External knowledge synthesis becomes part of the triangle when it stops being asked to do work it cannot do. The external engine is the part of the answer that draws on the global evidence base. It is the necessary partner to the chart corner (patient context) and to the internal knowledge corner (institutional context). The most thoughtful vendors are already framing themselves this way i.e. as one input into a larger architecture, not as the whole architecture.
When external knowledge engines integrate cleanly with internal knowledge engines, the triangle gets significantly closer to being whole.
How this health system works.
Internal knowledge synthesis is the AI answer engine for everything that is true about how this health system practises. Local protocols. Local formularies. Local pathways. Local referral routes. Local diagnostic and imaging access. Local consultant preferences. Local approved deviations from national guidance. Local antimicrobial stewardship policies. Local resistance patterns. Local equipment. The accumulated, governed, hospital-specific knowledge that turns "what is generally recommended" into "what we actually do here."
The least developed part of the triangle. Almost every health system has tried to solve internal knowledge with the tools it already had i.e. SharePoint, intranets, shared drives, custom portals, occasionally a dedicated policy management system. None of them were built for the way clinical care actually happens, and all of them suffer from the same fatal symptom: clinicians do not use them. A guideline no one reads cannot reduce variation. A protocol no one finds cannot improve outcomes. An audit trail no one populates cannot defend a clinician in a coroner's court.
A small number of platforms are building purpose-built internal knowledge management for healthcare. The category is in the early adopters phase of adoption but is rapidly expanding.
Internal knowledge is structurally the hardest part of the triangle, which is why it has taken longest to arrive.
The content itself is messy. Where the global medical literature is curated, structured, indexed, peer-reviewed and growing predictably, a health system's internal knowledge is fragmented across PDFs, intranets, drives, and clinicians' heads. There is no editorial board. There is no standard taxonomy. There is no API. Important guidance is written by clinicians who have day jobs and review cycles measured in years.
Governance is the second limit. Internal knowledge changes constantly. Guidelines committees meet quarterly. New national guidance is released and has to be locally adapted. Drug shortages and formulary changes happen weekly. An internal knowledge platform that doesn't have rigorous version control, approval workflows, and a clear "which version is in force" answer at any given moment is unsafe to use clinically.
Adoption is the third limit and the largest. Clinicians do not log in to stand alone portals. They do not read intranet announcements. Any internal knowledge platform that lives on a desktop, requires a separate login, or asks for time the clinician does not have will fail and most of them have. This is why the SharePoint generation of internal knowledge tools has been so consistently disappointing. The technology was never the limit. The form factor was.
And there is a fourth limit specific to this corner: nobody outside the institution can solve it for you. External knowledge is licensable; OpenEvidence and UpToDate can race because they all draw from broadly the same global corpus. Internal knowledge has to be ingested, structured, and governed per hospital. Every health system is its own corpus. That is why it is structurally hard. It is also why it is structurally defensible: once a platform has ingested a hospital's internal knowledge, the data layer underneath becomes one of the most defensible assets in clinical AI.
Internal knowledge synthesis becomes part of the triangle when four things happen.
First, the content layer is ingested at scale i.e. protocols, guidelines, SOPs, formularies, calculators, equipment manuals, education and “tacit knowledge” - without manual tagging, without an IT project, without rebuilding the health system's governance from scratch. Automated content onboarding is now becoming feasible with the current generation of AI.
Second, the platform is governed natively. Approval workflows, version control, audit trails, and clinical sign-off have to be built into the architecture, not bolted on. This is where most policy management software historically fails.
Third, the platform delivers at the point of care. Mobile, fast, citation-grounded, used in the clinician's pocket at triage, in resus, in the clinic and on the ward. Not behind a portal login. Not via email bulletins. The form factor is the adoption story.
Fourth, the platform integrates with the rest of the triangle i.e. receiving conversation context from the ambient corner, patient context from the chart corner, and the world's evidence from the external knowledge corner so the answer it gives is informed by every relevant input.
If you lead clinical AI strategy in a health system, the Golden Triangle implies four things.
The triangle is the procurement frame, not any single corner. Most health systems are evaluating ambient AI, chart copilots, external knowledge engines, and internal knowledge platforms as separate procurement processes, run by different teams, on different timelines. The integrated future does not work that way. Ask every vendor: which corner do you own, and how do you integrate with the other three. The vendors that answer that question clearly will be the ones still in your stack in 2030.
No corner is "the solution." All are necessary. Beware of any vendor that claims to span all four corners (at least at this stage of clinical AI, who knows….maybe someday the triangle will be monopolised?). The structural advantage in clinical AI is not going to the company trying to do everything. It is going to the company that owns one corner well and integrates honestly with the other three. A triangle of best-in-corner platforms, integrated through open standards and shared context, will beat any single-vendor stack on every dimension that matters.
The internal knowledge corner is the unsolved half. Most health systems today are investing heavily in conversation and chart, less in external knowledge (because they assume OpenEvidence or UpToDate is "handled"), and almost nothing in internal knowledge. This is the wrong allocation. Internal knowledge is the corner that will most directly close the gap between what your clinicians have access to and what they actually do at the bedside. Without it, the rest of the triangle delivers excellent documentation and excellent search but not better care.
Plan the architecture, then buy the components. The health systems that move first on the Golden Triangle will be the ones whose CMIO, CMO, CNIO, CNO and Chief Pharmacist sit down together and design the architecture before they buy any single component. The ones that wait will inherit whichever architecture happens to consolidate around them and will discover too late that they don't own the corners that matter most.

%201.svg)
%201.svg)



